Antibody Graves Disease Pregnancy . Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Therefore, to predict fetal or neonatal hyperthyroidism, the most Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still.
from www.bio.davidson.edu
Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Therefore, to predict fetal or neonatal hyperthyroidism, the most Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of.
Graves Disease
Antibody Graves Disease Pregnancy The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Therefore, to predict fetal or neonatal hyperthyroidism, the most
From www.dreamstime.com
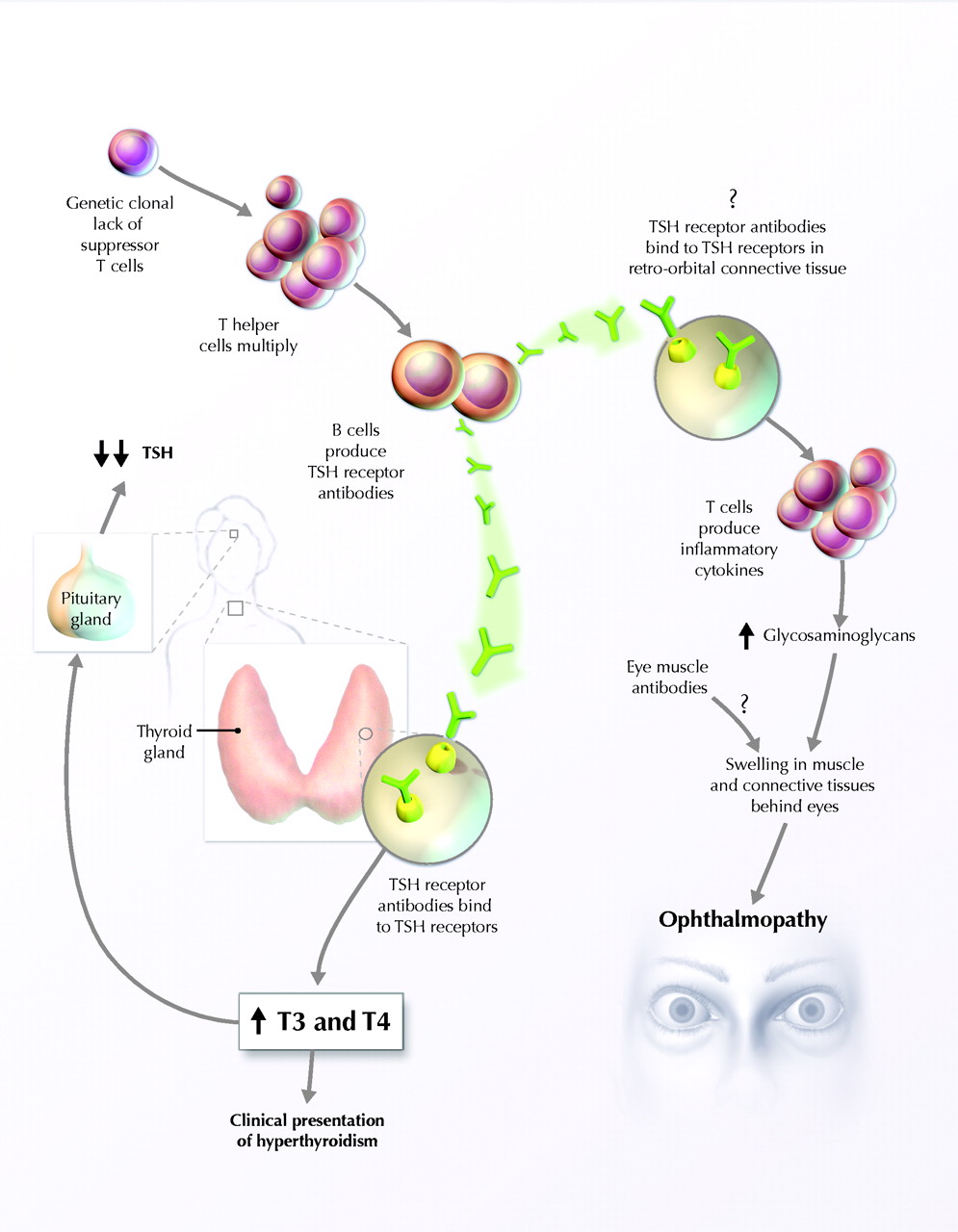
Illustration of the Graves Disease Causes. Vector Scheme Showing Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. The ata guidelines on pregnancy and the postpartum note that. Antibody Graves Disease Pregnancy.
From askthenurseexpert.com
Understanding Graves Disease Ask The Nurse Expert Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Antibody titers decrease in the second half of. Antibody Graves Disease Pregnancy.
From www.intechopen.com
Pregnancy in Women with Graves’ Disease Focus on Fetal Surveillance Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. The ata guidelines on. Antibody Graves Disease Pregnancy.
From www.whythyroid.com
Graves' Disease Causes, Symptoms, Diagnosis, Treatment Why Thyroid Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Therefore, to predict fetal or neonatal hyperthyroidism, the. Antibody Graves Disease Pregnancy.
From www.frontiersin.org
Frontiers Criminal of Adverse Pregnant A Perspective From Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period. Antibody Graves Disease Pregnancy.
From journals.sagepub.com
Hyperthyroidism During Pregnancy Etiology, Diagnosis and Management Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Therefore, to predict fetal or neonatal hyperthyroidism, the most The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared,. Antibody Graves Disease Pregnancy.
From www.cmaj.ca
Diagnosis and management of Graves' disease CMAJ Antibody Graves Disease Pregnancy The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the. Antibody Graves Disease Pregnancy.
From www.slideserve.com
PPT Outline PowerPoint Presentation, free download ID158539 Antibody Graves Disease Pregnancy Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the. Antibody Graves Disease Pregnancy.
From www.researchgate.net
Summary of Concerning Management of Graves' Disease in Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). The ata guidelines on pregnancy and the postpartum note that women with graves' disease during. Antibody Graves Disease Pregnancy.
From www.youtube.com
Thyroid Disease in Pregnancy Part 4 The Management of Graves Disease Antibody Graves Disease Pregnancy The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Therefore, to predict fetal or neonatal hyperthyroidism, the most Treatment of graves disease in pregnancy. Antibody Graves Disease Pregnancy.
From pregnancylinese.blogspot.com
Thyroid Eye Disease Icd 9 Pregnant Center Informations Antibody Graves Disease Pregnancy The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Therefore, to predict fetal or neonatal hyperthyroidism, the most Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can. Antibody Graves Disease Pregnancy.
From www.dreamstime.com
Grave`s Disease Cause. Antithyroid Antibodies Stock Vector Antibody Graves Disease Pregnancy The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Antibody titers decrease in the. Antibody Graves Disease Pregnancy.
From www.slideserve.com
PPT Hyperthyroid in Pregnancy PowerPoint Presentation, free download Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Therefore, to predict fetal or neonatal hyperthyroidism, the most Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered. Antibody Graves Disease Pregnancy.
From healthcare.utah.edu
Graves’ Disease Eyes (Thyroid Eye Disease) John A. Moran Eye Center Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Therefore, to predict fetal or neonatal hyperthyroidism, the most Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy,. Antibody Graves Disease Pregnancy.
From fyofwezds.blob.core.windows.net
What Is The Graves Disease Antibody at Rafael Hardiman blog Antibody Graves Disease Pregnancy Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Therefore, to predict fetal or neonatal hyperthyroidism, the. Antibody Graves Disease Pregnancy.
From www.bio.davidson.edu
Graves Disease Antibody Graves Disease Pregnancy Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have. Antibody Graves Disease Pregnancy.
From pregnancysymptomslove.blogspot.com
Symptoms Of Graves Disease During Pregnancy pregnancysymptoms Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause. Antibody Graves Disease Pregnancy.
From exobsegqz.blob.core.windows.net
Graves' Disease Antibody Test at Lucinda Murphy blog Antibody Graves Disease Pregnancy The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Therefore, to predict fetal or neonatal hyperthyroidism, the most Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by. Antibody Graves Disease Pregnancy.
From exobsegqz.blob.core.windows.net
Graves' Disease Antibody Test at Lucinda Murphy blog Antibody Graves Disease Pregnancy Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period ().. Antibody Graves Disease Pregnancy.
From www.momjunction.com
How To Diagnose And Treat Graves' Disease In Children? Antibody Graves Disease Pregnancy Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled.. Antibody Graves Disease Pregnancy.
From myendoconsult.com
Graves Disease And Pregnancy My Endo Consult Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Therefore, to predict fetal or neonatal hyperthyroidism, the most The circulating maternal thyrotropin receptor antibodies in graves’ disease. Antibody Graves Disease Pregnancy.
From www.osmosis.org
Graves disease Clinical Sciences Osmosis Video Library Antibody Graves Disease Pregnancy The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. The ata guidelines on. Antibody Graves Disease Pregnancy.
From www.osmosis.org
Graves disease Video, Anatomy, Definition & Function Osmosis Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Therefore, to. Antibody Graves Disease Pregnancy.
From www.cureus.com
ThyroidStimulatory Antibody as a Predictive Factor for Graves’ Disease Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. Therefore, to predict fetal or neonatal hyperthyroidism, the most Treatment of graves disease in pregnancy requires careful consideration of the. Antibody Graves Disease Pregnancy.
From pregnancysymptomslove.blogspot.com
Symptoms Of Graves Disease During Pregnancy pregnancysymptoms Antibody Graves Disease Pregnancy Therefore, to predict fetal or neonatal hyperthyroidism, the most Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy,. Antibody Graves Disease Pregnancy.
From www.mdpi.com
IJMS Free FullText Characterizing the Interplay of Lymphocytes in Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period. Antibody Graves Disease Pregnancy.
From movementdisorders.onlinelibrary.wiley.com
Thyroid Disorders and Movement Disorders—A Systematic Review Antibody Graves Disease Pregnancy The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross the placenta and cause fetal. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during. Antibody Graves Disease Pregnancy.
From fyofwezds.blob.core.windows.net
What Is The Graves Disease Antibody at Rafael Hardiman blog Antibody Graves Disease Pregnancy Therefore, to predict fetal or neonatal hyperthyroidism, the most Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Mothers taking antithyroid drugs in pregnancy may also present late, once the. Antibody Graves Disease Pregnancy.
From diseases-club2.blogspot.com
tsh in graves disease Tsh antibodies disease receptor diagnosis Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. Therefore, to predict fetal or. Antibody Graves Disease Pregnancy.
From exobsegqz.blob.core.windows.net
Graves' Disease Antibody Test at Lucinda Murphy blog Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period. Antibody Graves Disease Pregnancy.
From www.pnas.org
Targeting fibrocytes in autoimmunity PNAS Antibody Graves Disease Pregnancy Therefore, to predict fetal or neonatal hyperthyroidism, the most Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. The circulating maternal thyrotropin receptor antibodies in graves’ disease have the potential to cross. Antibody Graves Disease Pregnancy.
From fyofwezds.blob.core.windows.net
What Is The Graves Disease Antibody at Rafael Hardiman blog Antibody Graves Disease Pregnancy Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Therefore, to predict fetal or neonatal hyperthyroidism, the most Mothers taking antithyroid drugs in pregnancy. Antibody Graves Disease Pregnancy.
From labpedia.net
AntiThyroid Microsomal Antibody, AntiThyroid Peroxidase antibody Antibody Graves Disease Pregnancy Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period. Antibody Graves Disease Pregnancy.
From onlinelibrary.wiley.com
Current concepts regarding Graves’ orbitopathy Bartalena 2022 Antibody Graves Disease Pregnancy The ata guidelines on pregnancy and the postpartum note that women with graves' disease during pregnancy can have a relapse of. Mothers taking antithyroid drugs in pregnancy may also present late, once the maternal drugs have cleared, but the antibodies are still. Therefore, to predict fetal or neonatal hyperthyroidism, the most Antibody titers decrease in the second half of pregnancy. Antibody Graves Disease Pregnancy.
From www.youtube.com
CoMICs Episode 17 Graves’ disease during pregnancy YouTube Antibody Graves Disease Pregnancy Autoantibodies to thyroglobulin and thyroid peroxidase are common in the euthyroid population and are considered secondary. Antibody titers decrease in the second half of pregnancy because of immunomodulation of pregnancy, followed by a possible flare during the postpartum period (). Treatment of graves disease in pregnancy requires careful consideration of the adverse effects of uncontrolled. The circulating maternal thyrotropin receptor. Antibody Graves Disease Pregnancy.