In neurological assessments, the terms 'decorate' and 'decerebrate' describe distinct stages of brain response to injury—each critical for accurate diagnosis and patient care.
:max_bytes(150000):strip_icc()/VWH-MichelaButtignol-DecerebrateAndDecorticatePosturing-4000x2700-cd59bde629ef425f95c2a0f740aa2b24.png)
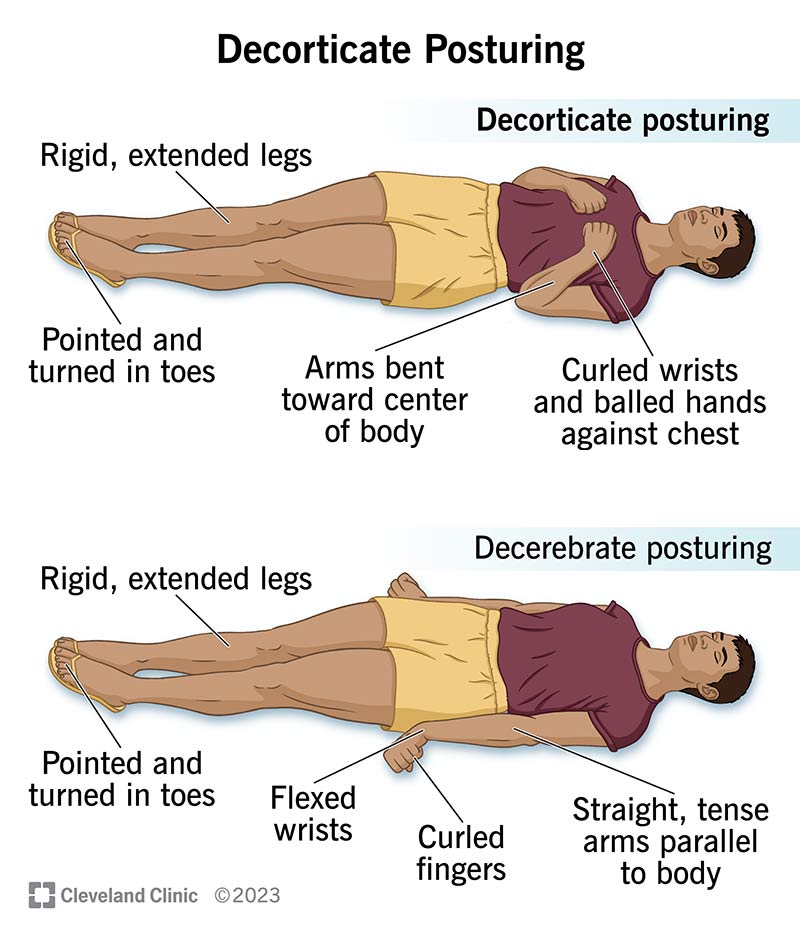
Decorate Status: Early Neurological Signs
Decorate refers to the initial phase of altered consciousness where motor responses resemble a decorative pattern—such as irregular, non-purposeful limb movements. This phase often indicates mild brain dysfunction and requires prompt monitoring to prevent progression to more severe states.
Decerebrate Posture: Advanced Neuronal Dysfunction
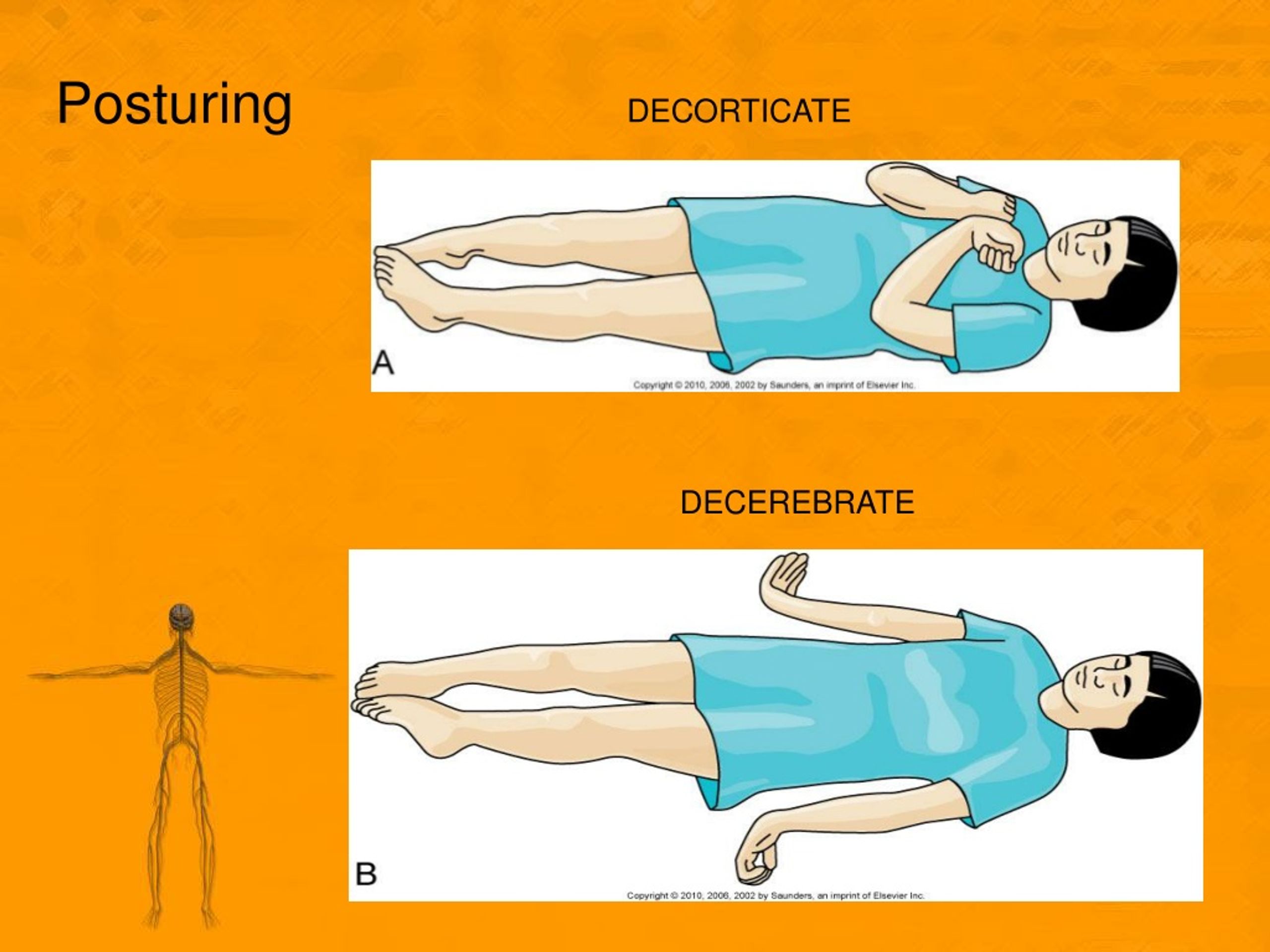
Decerebrate describes a severe neurological state characterized by rigid extension of the limbs and sustained posturing, reflecting extensive brainstem damage. This sign signals critical impairment and demands urgent medical intervention to manage complications.
Clinical Distinctions and Prognosis
Distinguishing between decorate and decerebrate states is vital for guiding treatment; while decorate may resolve with supportive care, decerebrate posture often indicates irreversible injury and a poorer prognosis. Accurate recognition ensures timely, targeted interventions.

Understanding the difference between decorate and decerebrate status empowers clinicians and caregivers to respond effectively to neurological emergencies. Stay informed to support better patient outcomes—early recognition saves lives.

Decorticate and decerebrate posturing results from brainstem dysfunction, such as in epilepsy or after a stroke. Learn what makes each position different. Here's a quick guide and helpful mnemonic on how to tell the difference between decorticate vs decerebrate and which is worse between the two.

Decorticate and decerebrate posturing are both considered pathological posturing responses to usually noxious stimuli from an external or internal source. Both involve stereotypical movements of the trunk and extremities and are typically indicative of significant brain or spinal injury.[1] The Nobel Laurette Charles Sherrington first described decerebrate posturing in 1898 after transecting. Learn how to recognize abnormal posturing (decorticate, decerebrate, and flaccid) for the NCLEX exam.
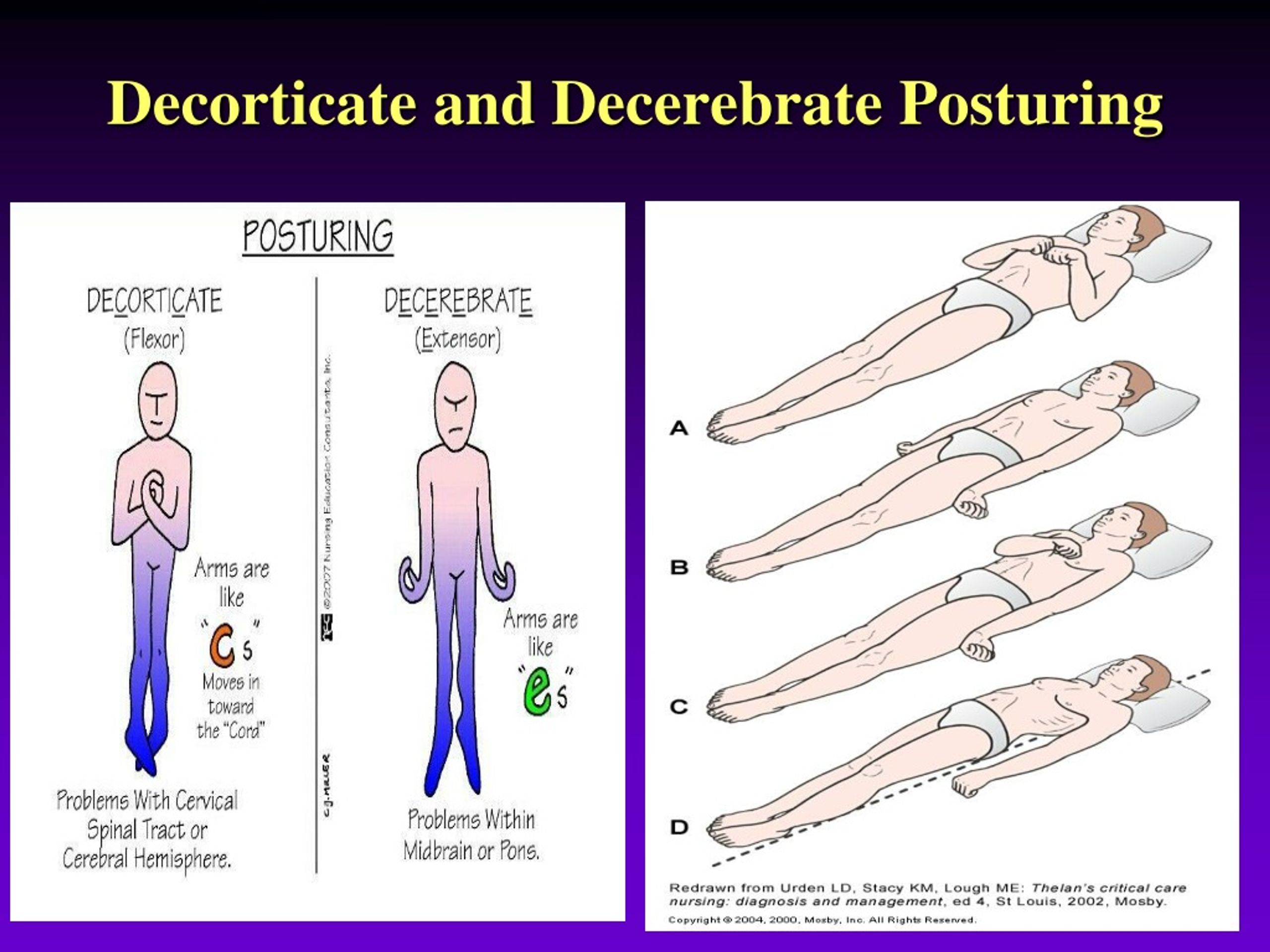
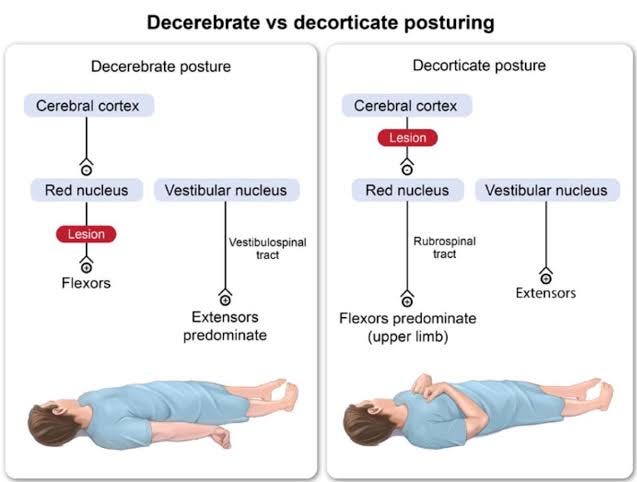
This guide breaks down key differences, clinical implications, and test. What Causes Decorticate and Decerebrate Posturing? Decorticate and decerebrate rigidity and posturing are the results of neurological damage usually due to traumatic brain injury or a non-traumatic brain injury such as a stroke. Specifically, upon decerebrate rigidity, caused when a lesion in the midbrain, pons, or diencephalon.

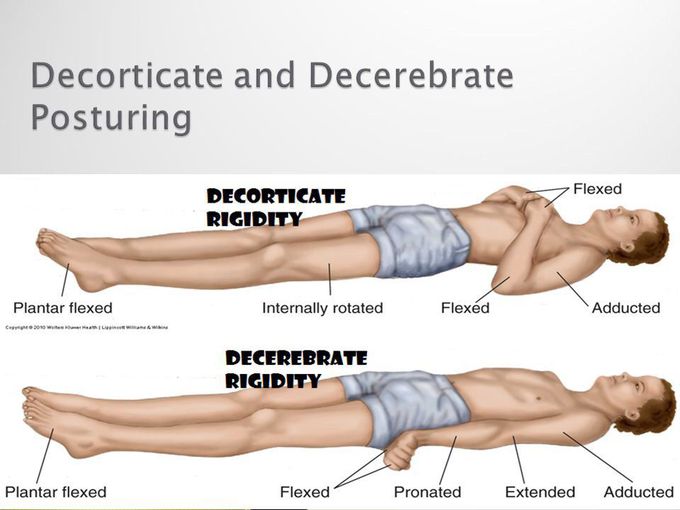
Decorticate and decerebrate posturing are abnormal body movements caused by brainstem disconnection from inhibitory cortical and subcortical pathways. As seen above, decorticate posturing (abnormal flexion to pain) and decerebrate posturing (extension to pain) score three and two points, respectively, for motor response. Decerebrate posturing is an abnormal body posture characterized by rigid extension of the limbs, while decorticate posturing is characterized by rigid flexion of the arms and extension of the legs.
Do you know that apart from normal postures or posturing, we also have postures that are abnormal like the decorticate posture or decerebrate posture? This article reviews the assessment and management of decorticate and decerebrate posturing and highlights the role of medical professionals in evaluating and treating patients with these conditions - abnormal postures. In this post, we will. Introduction Decorticate and decerebrate posturing are both considered pathological posturing responses to usually noxious stimuli from an external or internal source.